

Which Vaccines and Why? {Part 1}
Years ago, as one of the few dads lurking on the Baby Center vaccine board, I can’t tell you how often a concerned parent popped on the board and posted that question to the group: Which vaccines would you choose, and why? It was asked almost every single day, and several mothers would always respond with, “None at all.”
“None at all” isn’t the most helpful answer to give a new parent looking for information and I was always hoping to see a better explanation for why mothers felt the way that they did. This is the information I wished had been pinned to the top of the group under the heading, “Which vaccines and why?” 
First and foremost, a baby can’t really make antibodies until they are about 8 months old. No antibodies to natural infection and none to vaccination. Their bodies can’t even recognize a bacterial vaccine without that bacteria being bound to a toxin. I’m not going to get into complicated details on that, but I’ll say this much: it’s the reason the Hib and Prevnar 13 bacterial vaccines are “conjugates” and bound to toxins. Also, it’s the reason the DTaP vaccine is a combo shot—the tetanus toxin makes the bacterial pertussis portion work a little bit better.
This is why nurses have to administer vaccines three times in a row (2-dose priming + booster) to even produce a moderate artificial antibody response—it doesn’t work the first couple of times. In fact, acupuncturist Michael Gaetarecorded an immunologist in 2011 admitting at a conference that, “The vaccines are given at pediatric wellness visits, and the idea is that you are training the parent to bring their child in at all the pediatric wellness visits, and that it’s only the year visit that actually is truly important. But that for most parents you are not going to get them to bring their kid in if they don’t come in at two months, four months, and six months. And so it’s actually more of a training thing.”
Did you hear that? You are expected to bring your baby to the pediatrician at 2, 4, and 6 months of age and inject them with bacteria, viruses, preservatives, aluminum, and mercury— that do not even stimulate an immune response— just so that you get your training to take them to the doctor for the rest of their childhood. Isn’t that a kick in the head? Listen to that MP3; it’s all there.
Babies, especially breastfed babies, are naturally anti-inflammatory. I’m no expert on the boob juice but I know that they need their mother’s antibodies for daily protection from infection, and those same antibodies keep inflammation at bay. Ideally a baby would be breastfed for a least a year; 6 months at minimum. If you can’t breastfeed your newborn child, do you need to vaccinate to protect them? Vaccines are no substitution for breast milk. What if your child needs to go to daycare at 3 months old—should you vaccinate out of fear? An unvaccinated infant is healthier than a vaccinated one with a fever and runny nose who’s fighting off 4 viruses and 5 different types of bacteria being injected into their muscles every-other-month. If you’re unable to breastfeed there are both formal and informal organizations for you to obtain donor milk for the first months of your baby’s life; just ask around in a crunchy mother group or your local Le Leche League.
What if you need to return to work at 6 weeks postpartum? Moms, let’s be honest: if you’ve been at your job for one year at a company with at least 50 employees, you are entitled to 12 weeks of unpaid maternity leave. Save up and take it. States like California have disability insurance that will give you even more time off, some of it paid. Go talk to your HR department or call your state services about what your options are. Don’t cut your maternity leave short and put a newborn into daycare. Babies should be protected at home with mommy—or daddy if the case may be, if mommy has a pump, which she gets for free from Obamacare.
This all means you should wait until a baby is at least 8 months old to begin vaccinations, if you decide vaccinations are right for your child. Bear in mind, though, that a body is never too old for a serious vaccine injury. I have seen an otherwise typical child regress into autism at 5 years old, and I know medical workers who have become disabled after Hepatitis B and flu vaccines. I know an adult male who became a quadriplegic after the flu vaccine just before Christmas and another that had tremors for weeks. Sure, all of that is rare, but when it’s your child that the rare reaction strikes, I bet it’s suddenly hard to argue the benefits outweigh the risks.
If you do decide that vaccines are right for your children, only allow one at a time every 60 days, breaking up the Pentacel (DTaP/polio/Hib combo vax) into separate shots, so that you can watch for reactions. The advantage to waiting all the way until 12 months to begin vaccinations is that you are confident in knowing your own child. They are probably saying “mama” and “dada,” they are pointing to objects they want. Some babies are walking by that age, they are learning to play appropriately with toys, and interacting with family. If your child loses any one of these milestones after receiving a vaccine, or starts to bang their head, have staring spells, seizures, or engage in repetitive behavior, it will be easy to recognize.
By 12 months old you might know if your child has food allergies or unusually sensitive skin, which point to autoimmune disease and a contraindication to vaccination, despite what the CDC says. Maybe by 12 months you will have paid for a genetic test like 23andMe and have found out if your child has an MTHFR mutation, which plays into their ability to process and excrete aluminum and mercury. Don’t believe that all vaccines are free of mercury. Some have a small drop, but the flu vaccine has 25 times that amount. Plus, aluminum is in the DTaP, Hib, Hep A, Hep B, and Prevnar 13 vaccines. If your doctor tries to tell you that any side effects, new illness or lost milestones are a coincidence, you will know better because you’ll know your baby. Besides, if you have a doctor that lies to your face, you should probably find a new doctor.
If you’re the type who wants a quick and dirty education on vaccines and doesn’t have time to do years of research, streaming a movie like The Greater Goodfor 5 bucks might be the right move for you, or get it for free on Hulu.
Let’s tackle 3 of the vaccines on the routine infant immunization, shall we?
Hepatitis B at birth and infancy: this one is a no-brainer. If there is one vaccine that parents suspect is unnecessary for a baby, it’s Hep B. Hep B is a blood-borne virus that is typically caught through vaginal sex, anal sex, used tattoo needles, and sharing drug needles. For whatever reason, living in Alaska is also a risk factor. The virus can live outside of the body for up to a week but is easily cleaned up with bleach and water. It does not cross the skin barrier—skin must be broken for it to enter. It is not a disease picked up on the playground unless a rare Hep B-positive child is bleeding all over the slide. It is not picked up on a toilet seat unless a Hep B-positive woman has… you get where I’m going. Hep B doesn’t cross the placenta so Hep B-positive mothers do not give Hep B to their children through pregnancy alone, although they can during birth. In this day and age I don’t know how a woman with Hep B could go through routine prenatal care and not know that she has Hep B.
There are only about 3,000 new symptomatic Hep B infections each year—compare that to 50,000 new HIV infections. Would you give your newborn an HIV vaccine if one was offered? Probably not, because vaccinating a newborn for a sexually transmitted disease is bizarre.
There is no denying that the beginning of several US epidemics coincide with the 1991 CDC recommendation of vaccinating day-old infants for Hep B, including autism and food allergies. Prior to 1991, babies were a full two months old before receiving a first vaccination. Chinese parents lost at least a dozen babies following Hep B vaccination in 2013 (all ruled to be coincidences), and Vietnam pulled Hep B lots from use after 3 infant deaths.
The CDC doesn’t even know how many Hep B-positive children there are; it is that small of a number. Have I heard of a Hep B-positive parent giving an infection to a child through sharing a toothbrush? Yes, I have. There are many reasons why you should not share toothbrushes with your child; that is just one of them. Do I think the Hepatitis B vaccine is important for at-risk adults? Sure, but adults aren’t lining up to receive it.
The Hepatitis B vaccine is one that you might consider for your child as they enter high school and/or become sexually active but only if they do not show any signs of having an autoimmune disease that would be worsened with vaccination. If you decide for them to receive the vaccine at 14, know that it will wear off by the time they graduate college. Lastly, be warned that the Hep B vaccine is suspected of causing the autoimmune disease multiple sclerosis from time to time.
RotaTeq at 2, 4 and 6 months: When was the last time you saw on the news that an American baby had died from diarrhea? Never? If your pediatrician tries scaring you with the half million deaths from rotavirus each year, tell them that while your heart aches for the babies of Africa, you do not base vaccine decisions for your child on tragedies half a world away. Keep it local. Besides, actively breastfed babies almost never contract rotavirus. However, that first dose of RotaTeq is known to shed in bowel movements for over a week, so your daycare baby could possibly infect other children through the vaccine. The maximum age to receive the rotavirus vaccine is 8 months so if your child reached that age without getting the vaccine, don’t lose any sleep over it. Besides, any child that comes down with rotavirus will get over it in a few days, many diapers, and dozens of baths later. Keep them hydrated and give an extra infant probiotic.
DTaP at 2, 4, 6 and 15 months: Pertussis, or whooping cough, is probably the scariest of the vaccine preventable diseases for an infant. In 2012, 18 childrendied of pertussis infection. From January 1992 to June 1995 when the more effective whole cell DTP was in use (DTaP replaced it in 1997), there were 32 pertussis deaths, which comes out to 21 deaths per year. If, in 20 years, the number of children who die from pertussis has remained unchanged, regardless of using DTP or DTaP, what does that tell us about the vaccine? At this point, the vaccination campaign is not saving additional lives. The lives lost to pertussis has remained constant for the last two decades, despite the declining vaccination rate and the transition to a less effective vaccine.
Is the vaccine creating a pertussis super bug? Is the disease worse than it used to be? Why can we accept that using antibiotics, antibacterials, and products containing triclosan all cause bacteria to mutate and become stronger, but we don’t apply the same logic to vaccinating for a bacteria?
In fact, the DTaP doesn’t even stop transmission of pertussis. Israeli researchers knew in the year 2000 that fully vaccinated children carry the pertussis bacteria without showing symptoms—something FDA researchersreconfirmed with baboons in 2013. This means that you think you’re doing the right thing by getting that Tdap before leaving the maternity ward, and asking family members to get a booster before visiting your newborn, but you might be doing more harm than good. You could very well be bringing asymptomatic pertussis infection into your house and exposing it to your newborn. You might be better off knowing when someone is sick and telling them not to come over.
What are your odds of catching pertussis? There were 48,000 cases in 2012. In the United States that’s less than a 1 in 6,500 chance of catching it. Is the 100-day cough a nightmare to deal with? For many people it is; for some people it’s not. A lot depends on the state of your health at the time you come down with it. There are stories of lost lung capacity or permanent cough from pertussis, especially if the person already had asthma. Vitamin C deficiency has long been thought to impair the body’s ability to defend against pertussis. Likewise, for at least 80 years large doses of vitamin C in the early stages of infectionhave also been used as a treatment to shorten the pertussis cough to anywhere between 5 and 15 days. Doctors are allowed to prescribe natural therapies like intravenous vitamin C, even in the hospital. Make sure you already have a holistically-minded one in your life if you want an infection treated that way.
The fact is this: babies are almost never, ever killed by pertussis over the age of 3 months old. We can’t say on one hand that’s because of the success of the DTaP vaccine and then say on the other that the DTaP is not very effective and that we need constant boosters to keep it under control. Keep your baby at home for the duration of your maternity leave, or longer if you can. Don’t take them to the grocery store and don’t even think about taking them to Disneyland.
Regardless of whether you decide to vaccinate for pertussis or if you accidentally acquired it by natural infection, immunity to bacteria doesn’t last forever. A natural infection protects for up to 20 years, while the vaccine wanes in 5 to 10. Parapertussis sounds and feels a lot like pertussis, but there is no vaccine for it.
It has long been thought that the DTP and the newer DTaP vaccines were the most reactive of the infant schedule, causing encephalophy which is often ruled to be Sudden Infant Death (SIDS) at the time of death. Someone leaked the 1979 Wyeth “hot lot” memo after the whole cell DPT killed 11 babies in Tennessee, 9 of them from the same lot. They decided that, going forward, it was best to spread out vaccines from one lot so it wouldn’t be so easy to point the finger at DTP the next time a wave of newborns died a few hours after vaccination.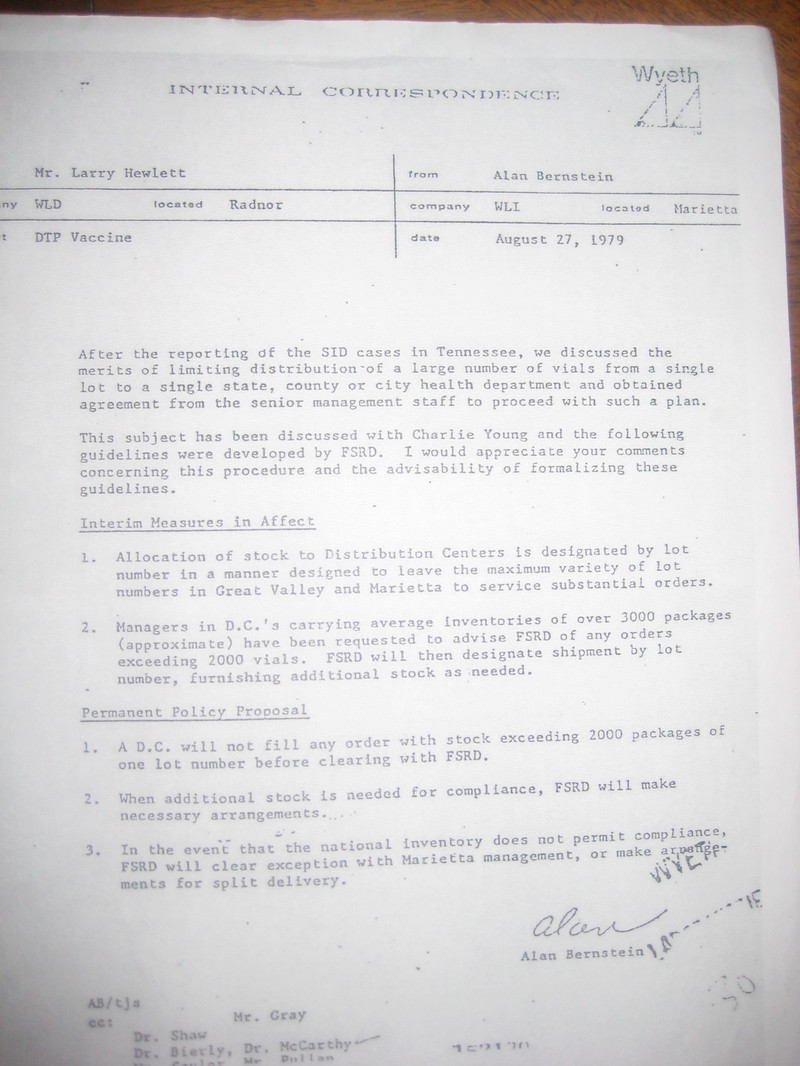 In 2010, there were 3,610 SIDS and Sudden Unexpected Infant Death (SUID) deaths. That comes out roughly to 1 out of every 1,000 children born that year. Compare those odds to your baby’s 1 in 6,500 chance of even catching pertussis and you decide if the benefits outweigh the risks.
In 2010, there were 3,610 SIDS and Sudden Unexpected Infant Death (SUID) deaths. That comes out roughly to 1 out of every 1,000 children born that year. Compare those odds to your baby’s 1 in 6,500 chance of even catching pertussis and you decide if the benefits outweigh the risks.
To be continued in Part 2 {more DTaP, Hep A, polio, PC}, Part 3 {Hib, MMR, CP, flu, HPV}.